

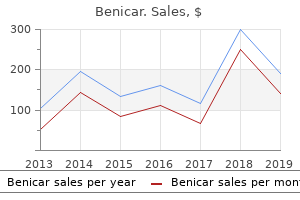
"Order benicar uk, blood pressure is high".
By: V. Tukash, M.B. B.CH., M.B.B.Ch., Ph.D.
Co-Director, Des Moines University College of Osteopathic Medicine
The frontal plane wire place ought to be consistent with the anatomic axis and proximally should be simply medial to the lateral tibial spine blood pressure monitor app buy cheap benicar 40mg online. Marking the pores and skin along the crest can help in aligning the guidewire with the path of the intramedullary canal and reduce the need for fluoroscopic steerage hypertension treatment safe 40mg benicar. Ideal proximal additional articular begin site as seen on lateral fluoroscopic picture; this is close to the articular margin hypertension and heart disease benicar 40 mg on line. An perfect insertion vector approaches a parallel path with anterior cortex and minimizes the probability of fragment extension with seating of the nail. Place a 15-degree bend 2 cm from the distal extent of the ball-tipped guidewire to permit for directional management during wire development. Alternatively, a straight ball-tipped guidewire can be used with an intramedullary reduction instrument (eg, a cannulated finger device), which might precisely direct the wire and simplify passage across the fracture. A ball-tipped guidewire is introduced into the proximal segment, and the knee is slightly prolonged for fracture reduction and instrumentation. Creating and Reaming the Starting Hole the opening reamer (matching the proximal nail diameter) is launched via a tissue sleeve and inserted while carefully maintaining knee hyperflexion and biplanar alignment. Fracture Reduction Simple Middle Diaphyseal Fractures (Transverse or Short Oblique) Manual traction with gross manipulation will reduce simple transverse mid-diaphyseal fractures. Medially-based exterior fixation or distraction with a big common distractor is useful for reduction when no assistants can be found, in large patients, or when used for provisional fixation. Placement of percutaneous pointed discount forceps could be helpful in indirect and quick oblique patterns to achieve anatomic or near-anatomic discount. Highly Comminuted Middle Diaphyseal Fractures Have comparability radiographic photographs of the unhurt extremity obtainable to be used as a template for length and rotational reduction landmarks. Use fluoroscopy to localize clamp position and determine ideal clamp incision locations. Percutaneous clamps can precisely reduce and stabilize indirect fractures before nail introduction. The intramedullary reduction software obtainable in most nail or reamer sets can be utilized to manipulate the proximal fragment to have the ability to advance the tool throughout the fracture which achieves fracture discount and guidewire placement. If discount is troublesome, a small-fragment unicortical plate can be used to maintain the reduction during reaming and nail placement. Passing the Guidewire Open Middle Diaphyseal Fractures Large segmental and butterfly fragments which are completely devitalized and void of soppy tissue attachments should be removed and cleaned of contamination. These pieces can then be reintroduced into the fracture website and used to carry out anatomic open reduction following passage of the intramedullary rod and interlocking. In metadiaphyseal fractures, the wire have to be centered within the metaphyseal phase. A half-pin positioned simply above the ankle joint lies below the projected finish of the nail. A massive segment of stripped cortical bone has been eliminated and cleaned on the back desk. The cortical fragment has been positioned into the fracture website and clamped in decreased place to cut back the fracture anatomically. Intraoperative image of the fracture with the fracture fragment clamped in reduced place; observe that this fragment will be removed after reaming and nail passage. A threaded end cap (usually 5, 10, and 15 mm) can be used if it is desired to bring the nail to top of the canal opening. A drill bit is used to ensure the guidewire is placed centrally in the distal section of this distal metadiaphyseal fracture. The nail length guide is pushed to the opening of the tibia and verified with lateral fluoroscopic imaging. The canal usually is reamed at least 1 mm over the isthmic diameter to minimize the risk of nail incarceration. Reamer heads must be evaluated before insertion and must be sharp and free of defects.
Care ought to be taken to maintain a bone bridge between recipient websites of 2 to 3 mm and to avoid recipient site convergence arrhythmia game discount benicar 20mg free shipping. In basic blood pressure chart record keeping purchase 40 mg benicar fast delivery, contact pressures are lower in the intercondylar notch and medial trochlea blood pressure pulse 95 generic benicar 40 mg visa, however out there harvest material is proscribed. The retropatellar fat pad is completely d�brided to improve visualization and keep away from delicate tissue entrapment. The perpendicularity rod should be inserted into this Harvester/Cutter assembly earlier than insertion into the joint. The perpendicularity rod will operate as an obturator and reduce both gentle tissue capture and fluid loss because the meeting is inserted into the knee. The Harvester Delivery Guide/Cutter/perpendicularity rod assembly is positioned on the donor site in preparation for the graft harvest. The perpendicularity rod is used to confirm the perpendicular place of the cutter and then eliminated. Perpendicular grafts may be obtained readily with each arthroscopic and open approaches. The T-handle of the harvester is rotated clockwise a minimum of two full rotations, undercutting the distal bone and making a exact harvest depth. On a agency surface, insert the Harvester Delivery Guide/ Cutter into the graft loader and push down firmly until it makes contact with the underside of the loader. Position the Harvester/Delivery Guide/Cutter with the perpendicularity guide on the chosen donor site. After verifying the perpendicularity, remove the guide after which tap the harvester till the specified laser line depth has been reached. This switch system eliminates any loads to the articular floor of the graft and eliminates the danger of chondrocyte injury on this step. The harvested graft might be pushed from the cancellous bone aspect of the graft plug upwards into the Harvester/Delivery Guide and out of the cutter part. The plastic plunger is placed in the harvester supply system before insertion of the delivery system into the joint. The loaded harvester�clear plastic delivery information system is then inserted into the knee. The eight mm facet is really helpful for 4 mm and 6 mm grafts and the 12 mm facet is recommended for eight mm and 10 mm grafts. A 2-mm to 3-mm bone bridge must be maintained between the drilled holes to enable for a safe graft press fit. Large-diameter and deep defects may cause excessive stress on the encircling cartilage and lead to degeneration. Maintain perpendicular orientation of the walls throughout recipient web site preparation to avoid unfastened plugs. Ensure that the recipient site is an applicable depth to avoid leaving a "proud" plug. In circumstances the place a plug is "angled" close to the encircling cartilage, the plug should be sunk so that the higher fringe of the graft is flush with the encircling surfaces. If the graft diameter is simply too massive, the recipient website may be "upsized" to the right width. If the graft is simply too small or unstable, an adjacent 4-mm tunnel may be prepared to wedge in the unique graft. Non�weight bearing is observed for 3 weeks, followed by progressive weight bearing throughout weeks 3 to 6 after surgery after which full weight bearing starting at 6 weeks after surgical procedure. Osteochondral transplantation persistently ends in restoration of hyaline cartilage versus "hyaline-like" or fibrocartilage. Multiple authors report wonderful and good results ranging from 78% to 96% at a minimal of two years followup. Biomechanical and topographic issues for autologous osteochondral grafting within the knee. A potential randomized medical study of mosaic osteochondral autologous transplantation versus microfracture for the remedy of chteochondral defects in the knee joint in young athletes. Dynamic analysis of contact pressure and the results of graft harvest with subsequent lateral launch at osteochondral donor websites within the knee. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and scientific expertise. Mosaicplasty for the treatment of articular cartilage defects: utility in medical apply.
The affected person must not externally rotate previous impartial (straight-ahead position) for six weeks arteria basilaris buy benicar 20mg overnight delivery. The patient is began on a passive stretching program that features passive external rotation with a cane as much as pulse pressure vs map purchase benicar 20mg online forty five levels and overhead stretches with a rope and pulley blood pressure chart chart cheap benicar amex. At 12 weeks from the operation the affected person is began on a strengthening program with elastic bands. If the subscapularis tear is part of a massive anterosuperior rotator cuff tear, then strengthening is delayed till 16 weeks postoperatively. Rehabilitation focuses on strengthening the scapular stabilizers and deltoid and rotator cuff muscular tissues. Eight of ten sufferers who had proximal humeral migration preoperatively had reversal of the migration and useful overhead use of their arm. Bennett2 also found encouraging results in his potential cohort with 2- to 4-year follow-up. Kim et al,9 in a current report of patients who had an arthroscopic repair of isolated partial articular-sided tears, discovered similar enhancements in pain and performance. Arthroscopic restore of isolated subscapularis tears: a prospective cohort with 2- to 4-year follow-up. Intra-articular restore of an isolated partial articular-surface tear of the subscapularis tendon. Rupture of the tendon of the lengthy head of the biceps brachii: surgical versus nonsurgical treatment. Incomplete tears of the subscapularis tendon related to tears of the supraspinatus tendon: cadaveric and clinical research. Histologic proof of degeneration at the insertion of 3 rotator cuff tendons: a comparative study with human cadaveric shoulders. Chapter 12 Repair and Reconstruction of Acromioclavicular Injuries Amir Mostofi, Augustus D. Dislocations are categorized by severity of harm, radiographic findings, and place of the clavicle12 (Table 1). Indirect damage happens by falling on an adducted outstretched hand or elbow, inflicting the humeral head to translocate superiorly and drive the humeral head into the acromion. The articular floor is made up of hyaline cartilage containing an intra-articular meniscus kind of structure, all surrounded by a joint capsule with a synovial lining. Appreciating the placement of the coracoclavicular ligament attachment on the clavicle is essential. The trapezoid attaches on the undersurface of the clavicle at an anterolateral place. Because of the innervation by the lateral pectoral nerve, some patients could present with anteromedial ache, additional complicating the image. Pain at posterior side of shoulder or lateral shoulder may indicate other pathology. Radiographs of the lateral finish of the clavicle may be slightly elevated, however stress views fail to show a one hundred pc separation of the clavicle and acromion. The higher extremity is usually held in an adducted place with the acromion depressed while the clavicle appears high-riding, however in reality the acromion and the the rest of the upper extremity is displaced inferior to the horizontal plane of the lateral clavicle. The distal clavicle is posteriorly displaced into the trapezius muscle and may tent the posterior pores and skin. Severe droop secondary to anteroinferior translation of the scapula across the thorax, because of the burden of the arm and the geometry of the chest wall. This is considered the third translation of the scapula with lack of the clavicular strut. The distal clavicle is found in two orientations, both subacromial or subcoracoid, behind the intact conjoined tendon. Mechanism is believed to be extreme hyperabduction and exterior rotation of the arm combined with retraction of the scapula. The conoid could be seen as a broad ligament that fans out, attaching to the clavicle in a posteromedial position. The width seen on radiographs is influenced by the individual variability of obliquity of the joint in relation to the x-ray beam. For optimal visualization of the acromioclavicular joint, the x-ray source is directed 10 levels cephalad with reduced penetration energy compared to a regular radiograph. It is helpful when a coracoid fracture is suspected with a traditional coracoclavicular interspace.
The nerve may be tracked throughout the ground of the supraspinatus fossa toward the spinoglenoid notch heart attack jokes discount benicar generic. The supraspinatus muscle may be evaluated and then retracted anteriorly heart attack 3964 generic benicar 40 mg visa, exposing the scapular backbone blood pressure chart dental treatment buy benicar cheap, which can then be followed to the spinoglenoid notch if evaluation for a constricting spinoglenoid ligament is important. This ligament can then be launched using a similar retraction approach on the nerve. The medial aspect of the coracoid base is used as a information to the suprascapular notch. Using the retractor to shield the artery, vein, and nerve will prevent inadvertent resection when utilizing the shaver or a punch. Using an excessive quantity of suction on the shaver pulls the nerve into the shaver owing to a vacuum effect and could minimize it. A lack of expert cadaveric apply in this process is a relative contraindication to trying the operation. Correct scapular position is crucial to restoration and will facilitate recovering regular energy. Although most sufferers see an instantaneous lower in ache and enhance in strength, it normally takes 6 to 12 months to regain normal strength in the infraspinatus and supraspinatus musculature. Therapy and electrical stimulation are continued until the patient can resume normal activities. The primary complication can be inadvertent nerve resection, however this has not been reported to our information. Suprascapular nerve palsy secondary to spinoglenoid cysts: outcomes of arthroscopic therapy. Chicago Il, March 2006, and on the American Orthopaedic Society for Sports Medicine Specialty Day. Arthroscopic launch of suprascapular nerve entrapment on the suprascapular notch: approach and preliminary outcomes. No substantial stories of arthroscopic spinoglenoid ligament launch had been discovered during our literature search. Nicholson has reported satisfactory results with open launch of the spinoglenoid ligament in a sequence of sufferers. There are principally two types of adhesive capsulitis that end in lack of vary of motion and may be safely addressed by arthroscopic releases: Primary adhesive capsulitis (idiopathic) Secondary adhesive capsulitis Associated with metabolic dysfunction (diabetes mellitus, thyroid disorder) Posttraumatic Postoperative Shoulder stiffness can result from intra-articular adhesions, capsular contracture, subacromial adhesions, and subdeltoid adhesions. The essential tenet of treating the stiff shoulder is recognizing the anatomic region liable for the stiffness and releasing the precise constructions in this region in a controlled style. An adequate appreciation of anatomy is essential to restoring movement and avoiding injury to accompanying tendons and nerves. Capsuloligamentous constructions contribute to stability of the shoulder joint and act as examine reins on the extremes of movement in their nonpathologic condition. During shoulder motion, tightening and loosening of the glenohumeral ligaments and capsule are accompanied by lengthening and shortening of the rotator cuff and deltoid muscular tissues. A plane between the deltoid and humerus (subdeltoid) exists that, when scarred, can restrict glenohumeral motion. A airplane between the rotator cuff and acromion exists and is occupied normally by a subacromial bursa. Several constructions that are essential to preserve are in continuity or proximity to the areas of the capsule which are released arthroscopically in the stiff shoulder. In their undiseased state they act as physiologic check reins at excessive ranges of movement. Fibrous bands can exist within the subacromial space (a) between the acromion and rotator cuff in addition to within the subdeltoid house (b) between the deltoid and rotator cuff or humerus. These can restrict tour of the rotator cuff and thus energetic and passive vary of motion. The axillary nerve runs throughout the superficial floor of the subscapularis after which adjacent to the inferior border of the subscapularis because it heads posteriorly. Anterior capsular launch can proceed safely as long as the muscle of the subscapularis is seen inferiorly. The posterior capsule overlies a definite layer of rotator cuff muscle posteriorly adjacent to the glenoid. The posterior rotator cuff tendons and capsule are juxtaposed and nearly indistinguishable more laterally. Release of the posterior capsule should be accomplished adjoining to the glenoid to avoid rotator cuff muscle and tendon disruption.
Cheap 10 mg benicar free shipping. Dr. Sarah Hallberg: How do electrolytes affect blood pressure on a ketogenic diet?.